
Mr. Chairman, and Members of the Committee, it is a great pleasure to be here today to share with you what we have been learning from science about the nature of drug abuse and addiction, and their prevention and treatment. Scientific advances supported by the National Institute on Drug Abuse (NIDA) are coming at an extraordinary rate and are significantly influencing the way this Nation approaches drug abuse and addiction. We are seeing science, rather than ideology, intuition, or common sense, beginning to drive the national discourse on these issues.
As you and members of this Committee are well aware, drug abuse and addiction take a tremendous toll on our Nation and their consequences are pervasive throughout every aspect of society. Drug use is a major factor in crime and delinquency, and in some communities, drug use is now the major vector for the spread of HIV/AIDS, tuberculosis and hepatitis. The good news in this grim and extremely costly scenario is that scientific advances both in the laboratory and in the clinical setting are providing us with tools to slow the drain of drugs on society. For purposes of today's discussion, my comments will be directed to all substances of abuse with the exception of alcohol, whose purview is that of another NIH Institute.
Research has brought us to the conclusions that drug abuse is a preventable behavior and that addiction is an eminently treatable disease. We have gained greater insight into why people use drugs in the first place. For example, we now know there are at least two major categories of drug users, and, importantly, they are clearly distinguishable. One group includes people who are simply novelty seekers, using drugs solely for their sensational effects. The second group is using drugs as if they are anti-anxiety or anti-depressant substances, trying to compensate for untreated mental disorders like depression or for terrible living situations such as dysfunctional families. The prevention and treatment approaches directed at each group differ significantly. For individuals self-medicating, for example, attention must be paid to the underlying mental disorder or emotional state, as well as to the substance of abuse. Similarly in prevention, messages must be developed that are targeted to the individual's motivation to use drugs.
We have learned in tremendous specificity the biological mechanisms by which drugs of abuse exert their psychoactive effects. Two decades of research have spelled out in great detail the brain mechanisms by which each drug of abuse changes mood, perception, or emotional state. Moreover, although each drug has its unique way of changing the brain, they all also share critical common characteristics. Virtually every drug of abuse, including nicotine, marijuana, cocaine, heroin, and methamphetamine, elevates levels of the neurotransmitter dopamine in the brain pathways that control the experience of pleasure.
Prolonged use of these drugs eventually changes the brain in fundamental and long-lasting ways, explaining why people cannot just quit on their own, why treatment is essential. In effect, drugs of abuse take over, or "highjack" the brain's normal pleasure and motivational systems, moving drug use to the highest priority in the individual's motivational hierarchy, which overrides all other motivations and drives. These brain changes, then, are responsible for the compulsion to seek and use drugs that we have come to define as addiction. Moreover, these brain and behavioral changes persist long after the individual has stopped using drugs. As one example, just last week, researchers reported in the American Journal of Psychiatry that methamphetamine abusers who were drug-free for up to eleven months still had significant memory and coordination deficiencies that were directly tied to brain changes produced by their prior drug use. (See figure below)
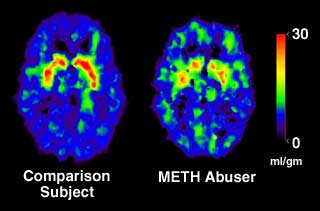 Source: Volkow, N.D. et al., Am J. Psychiatry, 158(3), pp. 377-382, 2001.
Source: Volkow, N.D. et al., Am J. Psychiatry, 158(3), pp. 377-382, 2001.Findings like these not only increase our understanding of addiction but also help point us to even more effective new treatments. In fact, NIDA has already developed and brought to the clinic an array of both behavioral and pharmacological treatments for addiction and has demonstrated their effectiveness in clinical trials. Numerous studies have shown that addiction treatments are just as effective as those for other illnesses. One very important analysis recently published in the Journal of the American Medical Association (JAMA, October 4, 2000) clearly shows that addiction treatments work just as well as treatments for other chronic, relapsing illnesses such as asthma, hypertension, and diabetes. In this analysis, treatment compliance, drop-out rates, and relapse rates were similar for all four diseases. In short, addiction treatment success rates are comparable to those for other chronic illnesses.
Our research also shows that comprehensive treatments that focus on the whole individual, and not just on drug use, have the highest success rates. These programs provide a combination of behavioral treatments, medications, and other services, such as referral to medical, psychological, and social services. The array of services provided must be tailored to the needs of the individual patient.
Scientific discoveries are also fueling the development of more successful strategies to deal with addicted criminal offenders. The core phenomenon is that untreated addicted offenders have extremely high rates of post-release recidivism both to drug use and to criminality. However, providing science-based treatments while offenders are under criminal justice control can dramatically reduce recidivism, again both to drug use and to later crime. Thus, understanding addiction as a treatable, chronic illness has beneficial ramifications for our national drug control efforts. The blended public health/public safety approach of dealing with addicted offenders benefits not only the patient, but the family and community as well.
Perhaps the most visible example of the blending of public health and public safety approaches can be seen by the growing number of drug courts that have been established over the years. More than 600 drug courts, which mandate and arrange for treatment, monitor progress, and arrange for other necessary services as needed, are currently operating across the country. NIDA is currently supporting research that is looking at the effectiveness of some of the different drug court approaches that are being utilized.
To truly reap the benefits of this blended public health/public safety approach it is imperative that we adhere to science-based principles of effective drug treatment. Not just anything called treatment will do. For example, studies in states such as Delaware and New York have shown that comprehensive treatment of drug-addicted offenders, when coupled with treatment after release from prison, can reduce drug use by 50 to 70% when compared to those who are untreated. Treated offenders are also 50-60% less likely to end up back in prison. These findings hold true for at least four years after release. However, if the after-care component is left out, the effects of in-prison treatment are dramatically reduced. In addition, the treatment provided must be comprehensive. It must attend to all the needs of the individual and help return him or her to becoming a fully productive member of society. This means that a continuum of care is crucial for success, including offering treatment and services to individuals as they transition to the community.
In the same way that we have developed and sent to the field general principles that define effective addiction treatment, we are now laying out the principles of effective corrections-based treatment which should be available within the year. In the interim, we recommend that the corrections systems use our widely acclaimed publication Principles of Effective Drug Addiction Treatment as a guide in developing and evaluating programs.
Research has also shown that drug addiction treatment programs that adhere to scientific principles benefit not only the patient and his immediate community, but the larger society as well. Besides reducing criminality, as I just mentioned, our studies have established that drug treatment reduces the spread of infectious diseases such as HIV and hepatitis C, and restores the ability of addicted individuals to be functioning, contributing members of society. Science-based treatments are also extremely cost effective, since they can save millions of dollars that would have been spent on the public health and safety consequences of drug abuse and addiction.
NIDA-supported science is not only helping us to deal with already addicted individuals, but is also steadily improving our ability to prevent the initiation of drug use. You may recall that in March 1997 we published the first-ever science-based guide to drug abuse prevention, Preventing Drug Use Among Children and Adolescents, that spelled out the principles that account for effective drug abuse prevention programs. Subsequent research has provided important details for effectively implementing those principles in diverse American communities and populations. Thus, we are currently updating the book to reflect new findings, and we plan to release it at our National Prevention Conference later this summer.
Advances in the prevention arena showing great promise to help prevent initial drug use are coming from researchers closely studying what makes people more susceptible or vulnerable to a potential drug problem. No single, unique factor determines which individuals will use drugs; rather, drug abuse appears to develop as the result of a variety of genetic, biological, emotional, cognitive, and social risk factors.
As researchers continue to identify risk and protective factors, the challenge becomes to understand how these factors interact to make individuals more or less vulnerable to not only initially trying drugs, but also abusing drugs and/or going on to become addicted to drugs.
As with treatment programs, tailoring prevention programs to an individual's needs is critical. For example, researchers who are specifically targeting programs to youth who may be more vulnerable to drug use are showing promising results. NIDA-supported scientists recently reported that they could reduce marijuana use among a targeted group of teens by focusing on their specific underlying emotional styles. We have learned that this kind of motivation-directed message targeting is critical to the success of prevention efforts. By developing and targeting prevention interventions such as public service announcements to specific teen personality-types who are sensation-seekers, researchers were able to reduce marijuana use by over 25%.
These research findings, which can help reduce the Nation's overall drug use, are being shared with the broadest audiences possible. NIDA has an aggressive media and education campaign to disseminate our research findings and to educate the public about what science is teaching us about addiction. One example of this can be seen in a recent outreach activity in which we developed and mailed a "NIDA Clinical Toolbox" to nearly 12,000 drug treatment programs around the country. The toolbox provides treatment professionals with a wealth of materials on new and effective approaches to help patients with drug-related problems.
Another example of how we are disseminating and sharing our research findings can be found in the way we have established our National Drug Abuse Treatment Clinical Trials Network (CTN). Through our CTN, which now consists of 14 research centers geographically distributed across the country who work with over 80 different community treatment providers, we are able to rapidly disseminate new research findings. Each Center, working with its partner community treatment providers, has established specially designed clinical research training programs and clinical education programs for local treatment providers. Because of the scope of the CTN, NIDA is confident it has created the infrastructure and enthusiasm that will enable the quickest implementation of new therapies and intervention strategies possible across the entire Nation. This clinical trials network will be central to achieving our millennial goal of improving the quality of drug abuse treatment throughout the Nation using science as the vehicle.
I hope the examples I have provided in this statement demonstrate NIDA's commitment to having science replace ideology, intuition and common sense as the primary basis for our national discourse on drug abuse and addiction. The advances that continue to emerge from our research portfolio are providing us with renewed hope that we will be able to prevent initial drug use and have a full clinical toolbox of treatments to offer those who do become addicted.
Thank you for the opportunity to testify before this Committee. I will be happy to respond to any questions you may have.